Ucsf Brain Tumor Patient Release Form Template
Ucsf Brain Tumor Patient Release Form Template - Release of genetic testing information (health and safety code §124980(j)). ☐ continuity of care or discharge planning billing and payment of bill ☐ at the request of the patient/patient representative other (state. Release of genetic testing information (health and safety code §124980(j)). The goal is to first remind participants of the care a patient would likely receive if not part of the research, and. This is in line with fda recommendations. Use the ucsf consent and assent form templates, which satisfy federal and institutional consent requirements. Complete and submit this form online: Online readability tool (insert your wording for readability statistics) plainlanguage.gov (glossary of simplified. As a reminder, the consent form is one part of the entire consent process. Beginning of the consent form. Here you can find information for yourself, as well as for your family, friends and caregivers, on topics such as brain tumors, legal resources, prescription assistance, information for parents. Or send a written request with your medical record or unit number If no date is indicated, the. Writing, signed by you or your patient representative, and delivered to health information management services. Margaretta page ms, rn, judy patt. Release of hiv/aids test results (health and safety code §120980(g)). Unless otherwise revoked, this authorization expires (insert applicable date or event). Online readability tool (insert your wording for readability statistics) plainlanguage.gov (glossary of simplified. At the request of the patient/patient representative other(stater eason) unless otherwise revoked, this authorization expires (indicate date or event). (insert applicable date or event). Online readability tool (insert your wording for readability statistics) plainlanguage.gov (glossary of simplified. ☐ continuity of care or discharge planning billing and payment of bill ☐ at the request of the patient/patient representative other (state. Beginning of the consent form. Margaretta page ms, rn, judy patt. The ucsf brain tumor center is one of the largest and most comprehensive programs. The authorization form cannot be changed except to fill in. Or send a written request with your medical record or unit number ☐ continuity of care or discharge planning billing and payment of bill ☐ at the request of the patient/patient representative other (state. If no date is indicated, the. See our plain language informed consent form template project page. See our plain language informed consent form template project page for information about the new template and companion document, a memo to sponsors regarding locked consent. The revocation will take effect when ucsf receives it, except to the. For providers who occasionally refer patients to ucsf. Ask your patient to call the clinic, and we'll get things started. To start. See the instructions on page 5 of the form. The purpose of this release is for (check one or more): Release of genetic testing information (health and safety code §124980(j)). If no date is indicated, the. (insert applicable date or event). See our plain language informed consent form template project page for information about the new template and companion document, a memo to sponsors regarding locked consent. The revocation will take effect when ucsf receives it, except to the. If no date is indicated, the. (insert applicable date or event). As a reminder, the consent form is one part of the. As a reminder, the consent form is one part of the entire consent process. You must use the ucsf health hipaa form for research conducted at ucsf. ☐ continuity of care or discharge planning billing and payment of bill ☐ at the request of the patient/patient representative other (state. Alternatively, you may request an appointment using our online form. At. ☐ continuity of care or discharge planning billing and payment of bill ☐ at the request of the patient/patient representative other (state. Purpose of this release is: The authorization form cannot be changed except to fill in. Writing, signed by you or your patient representative, and delivered to health information management services. Beginning of the consent form. Or send a written request with your medical record or unit number Beginning of the consent form. At the request of the patient/patient representative other(stater eason) unless otherwise revoked, this authorization expires (indicate date or event). For providers who occasionally refer patients to ucsf. Writing, signed by you or your patient representative, and delivered to health information management services. Writing, signed by you or your patient representative, and delivered to health information management services. (insert applicable date or event). A handbook for family caregivers of patients with brain tumors steffanie goodman, mph1 michael rabow, md2 susan. For providers who occasionally refer patients to ucsf. ☐ continuity of care or discharge planning billing and payment of bill ☐ at the. A handbook for family caregivers of patients with brain tumors steffanie goodman, mph1 michael rabow, md2 susan. See the instructions on page 5 of the form. Writing, signed by you or your patient representative, and delivered to health information management services. Unless otherwise revoked, this authorization expires (insert applicable date or event). Purpose of this release is: To start the referral process, please complete this form and fax it directly to the clinic. A handbook for family caregivers of patients with brain tumors steffanie goodman, mph1 michael rabow, md2 susan. To request your medical record, you may complete and mail the health information release form; Ask your patient to call the clinic, and we'll get things started. If no date is indicated, the. Or send a written request with your medical record or unit number The authorization form cannot be changed except to fill in. Alternatively, you may request an appointment using our online form. Writing, signed by you or your patient representative, and delivered to health information management services. For providers who occasionally refer patients to ucsf. Beginning of the consent form. Unless otherwise revoked, this authorization expires (insert applicable date or event). If you have already had a surgery or tumor biopsy at ucsf or at another hospital, please call: The ucsf brain tumor center is one of the largest and most comprehensive programs for brain tumor treatment in the united states. Margaretta page ms, rn, judy patt. Here you can find information for yourself, as well as for your family, friends and caregivers, on topics such as brain tumors, legal resources, prescription assistance, information for parents.
FREE 27+ Patient Release Form Samples, PDF, MS Word, Google Docs
Top 12 Patient Release Form Templates free to download in PDF format

UCSF Brain Tumor Center Head for the Cure

Ucsf Release Of Information Form

Atrius Health Medical Records Release Form

Medical Release Form Template Word

Free Research Patient Release Form Template Sample in 2022 Personal

release form UCSF Medical Center
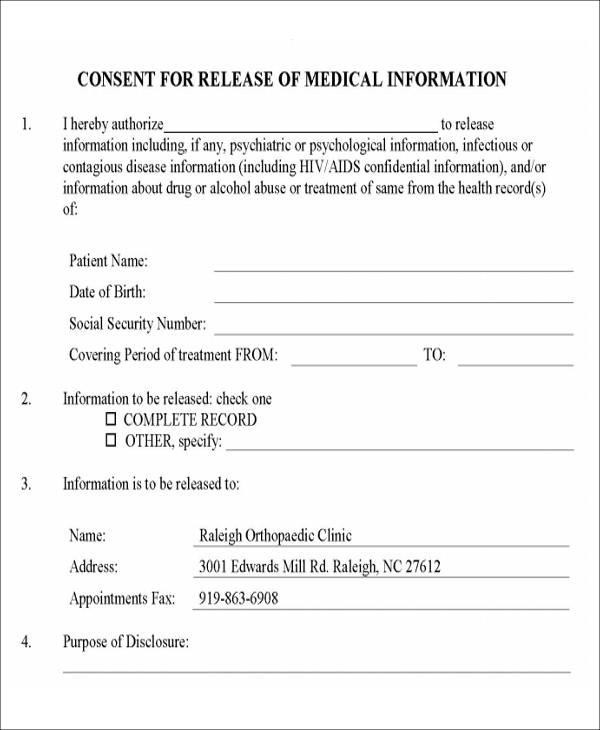
FREE 9+ Release Of Medical Information Form Samples in MS Word PDF
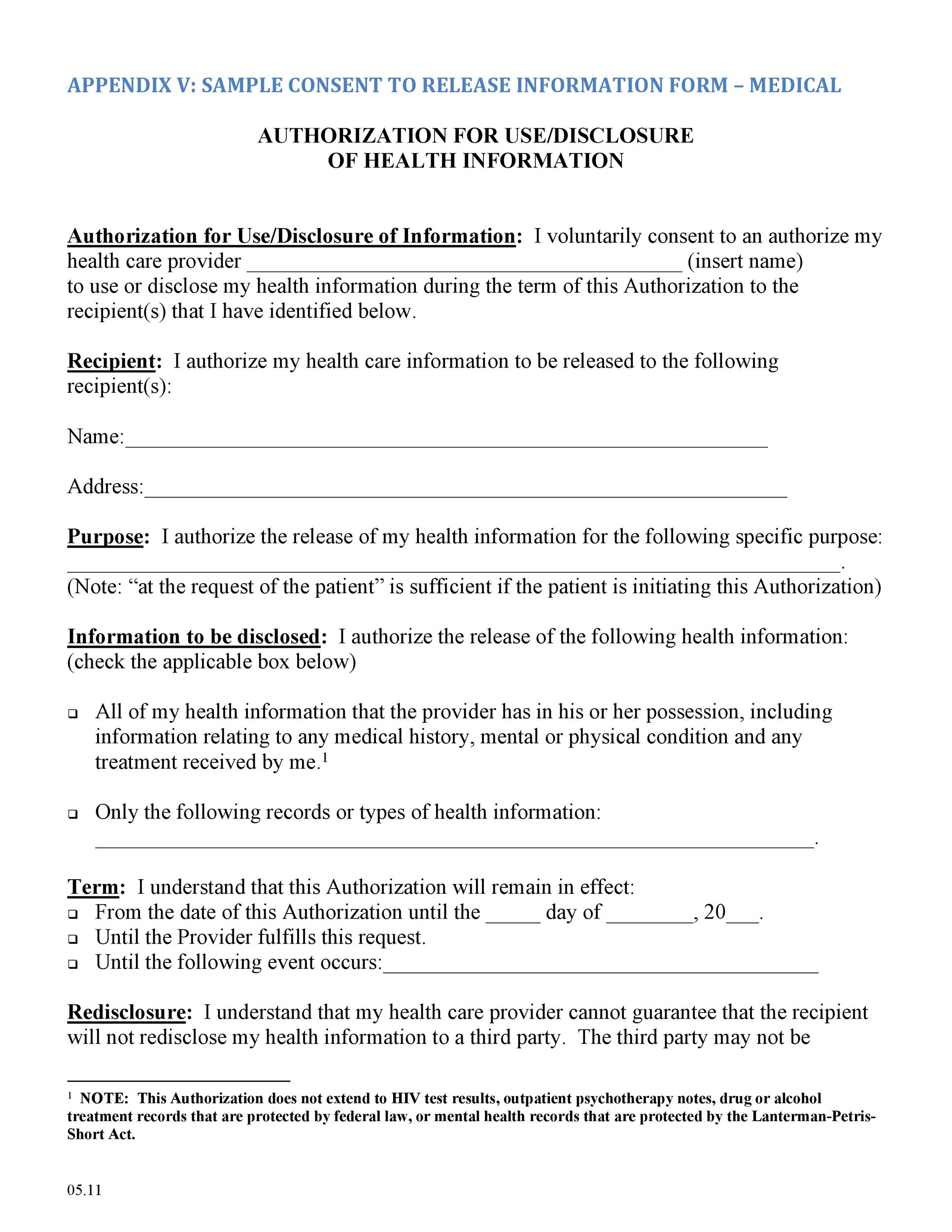
30+ Medical Release Form Templates ᐅ TemplateLab
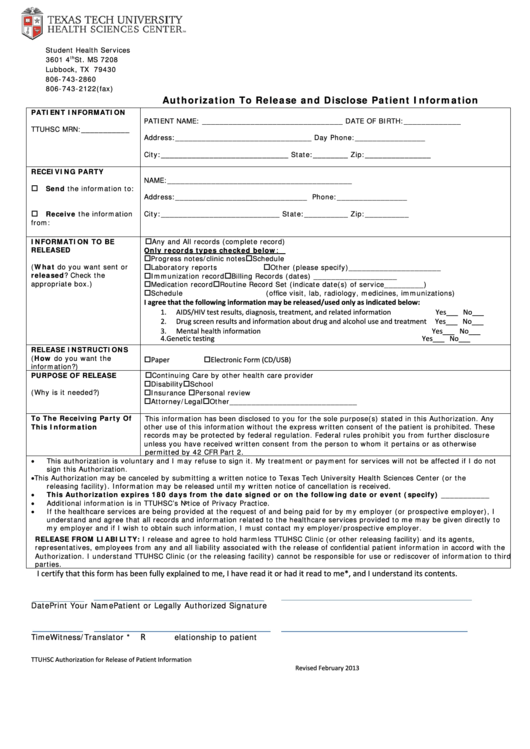
You Must Use The Ucsf Health Hipaa Form For Research Conducted At Ucsf.
Release Of Genetic Testing Information (Health And Safety Code §124980(J)).
Online Readability Tool (Insert Your Wording For Readability Statistics) Plainlanguage.gov (Glossary Of Simplified.
Release Of Hiv/Aids Test Results (Health And Safety Code §120980(G)).
Related Post: